- 1What Are the Stages of Lung Cancer?
- 2What Is Lung Cancer Staging and Why Does It Matter?
- 3How Do Doctors Determine Lung Cancer Staging?
- 4What Are the Stages of Non-Small Cell Lung Cancer?
- 5Staging Comparison Table: NSCLC Stages at a Glance
- 6How Is Small Cell Lung Cancer (SCLC) Staged?
- 7How to Find Out Your Lung Cancer Stage?
- 8When to Seek a Second Opinion on Staging
- 9Understand Your Stage, Then Ask the Right Questions
- 10Conclusion
- 11Key Takeaways
What Are the Stages of Lung Cancer?
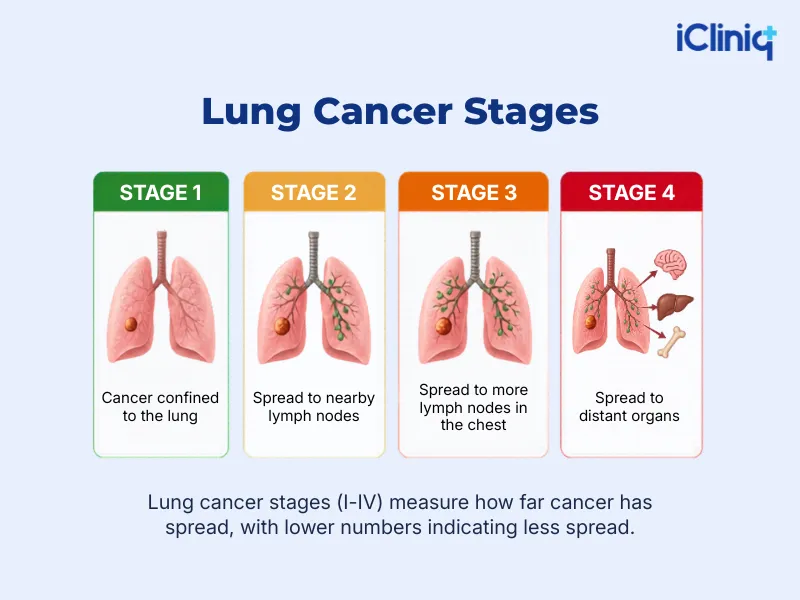
Lung cancer is staged on a scale from stage 1 to stage 4, based on how big the tumor is, whether it has spread and reached lymph nodes, and whether it has spread to distant vital organs. The stage at diagnosis directly shapes treatment options and expected outcomes. According to the American Cancer Society, around ~230,000+ new cases of lung cancer are diagnosed each year, making accurate staging one of the first and most critical steps after a diagnosis.
What Is Lung Cancer Staging and Why Does It Matter?
Staging is how doctors measure how far a cancer has progressed. For lung cancer specifically, the stage tells your care team three things: tumor size and location, whether nearby lymph nodes are involved, and whether the cancer has reached distant organs like the liver, bones, or brain. This information determines which treatments are appropriate. A stage 1 patient may be a candidate for surgery alone. A stage 4 patient may require a combination of chemotherapy, immunotherapy, or targeted therapy. Without an accurate stage, there is no clear treatment plan.
Staging also provides patients with a realistic picture of their prognosis. While no stage is a guarantee of any specific outcome, survival statistics by stage help patients and families make informed decisions.
How Do Doctors Determine Lung Cancer Staging?
The TNM Staging System
The most widely used staging system for NSCLC is the TNM system. It was developed and maintained by the American Joint Committee on Cancer (AJCC).
Each letter represents a different dimension of the cancer:
-
T (Tumor): Here, the main consideration is the size of the main tumor and how close it is to surrounding tissue. A T1 indicates the tumor is still small and contained, while a T4 indicates it has grown large or is pushing into nearby organs.
-
N (Node): This indicates whether cancer cells have spread to nearby lymph nodes. N0 indicates the nodes are clear, while N3 indicates the spread has reached nodes farther from the original tumor.
-
M (Metastasis): This simply answers one question: has the cancer traveled to other organs in the body? M0 means it has not, and M1 confirms that it has.
The combination of T, N, and M scores is then grouped into stages 1-4.
Doctors gather this information through imaging CT (computed tomography) scans, PET scans, and MRI along with biopsies and sometimes surgical exploration.
What Are the Stages of Non-Small Cell Lung Cancer?
Non-small cell lung cancer (NSCLC) is the most common form of lung cancer, making up around 85% of all diagnosed cases. It covers several subtypes, including adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. The staging system below applies to all NSCLC subtypes.
Stage 1 - Cancer Confined to the Lung:
At stage 1, the tumor is small and has not spread to nearby lymph nodes or to distant organs.
Stage 1 is divided into two sub-stages:
-
Stage 1A: Tumor is 3 cm or smaller and fully contained within the lung tissue.
-
Stage 1B: Tumor is between 3 cm and 4 cm, or has begun to involve the lung's inner lining but has not reached lymph nodes.
Typical Treatment: Surgery (lobectomy or wedge resection) is the standard approach. Stereotactic Body Radiotherapy (SBRT) is an option for patients who cannot tolerate surgery. The 5-year survival rate at this stage ranges from 60 to 80 percent, depending on the substage, according to the National Cancer Institute's SEER (Surveillance, Epidemiology, and End Results) database.
Stage 2 - Cancer Has Spread Locally:
At stage 2, the cancer may be larger or have reached nearby lymph nodes within the lung.
-
Stage 2A: Tumor is 4 to 5 cm and has not spread to lymph nodes, or a smaller tumor with limited lymph node involvement.
-
Stage 2B: The tumor size is 5 to 7 cm, or the cancer has reached the chest wall, diaphragm, or nearby tissue.
Typical Treatment: Surgery followed by adjuvant chemotherapy is the primary approach. Radiation therapy is added when margins are not clear. The 5-year survival rate is approximately 53-60% for Stage 2A and 35-46% for Stage 2B.
Stage 3 - Regional Spread:
Stage 3 is considered locally advanced. The tumor may be large, and the cancer has spread to the lymph nodes in the chest.
-
Stage 3A: Cancer in lymph nodes on the same side as the tumor, which may still be resectable in some cases.
-
Stage 3B: Cancer in lymph nodes on the opposite side of the chest or near the collarbone.
-
Stage 3C: Multiple tumors in the same lung with extensive lymph node involvement.
Typical Treatment: A combination of concurrent chemotherapy and radiation is the standard of care for most Stage 3 patients. Surgery may be appropriate in select Stage 3A cases. Immunotherapy after chemoradiation has shown meaningful improvement in progression-free survival in stage 3 patients, per clinical trial data posted in the New England Journal of Medicine.
Stage 4 - Metastatic Disease:
At stage 4, cancer has spread beyond the chest to other organs.
- Stage 4A: Cancer has spread to the opposite lung, fluid around the heart or lungs, or one distant organ.
- Stage 4B: Cancer has spread to multiple distant organs or locations.
Typical Treatment: Surgery is rarely an option at Stage 4. Treatment focuses on systemic therapies, chemotherapy, targeted therapy (for patients with EGFR, ALK, or ROS1 mutations), and immunotherapy. The 5-year survival rate for advanced (stage 4) lung cancer is generally reported in the single digits in population studies, although outcomes are improving for patients with specific targetable mutations.
Staging Comparison Table: NSCLC Stages at a Glance
|
Stage |
Tumor Size |
Lymph Nodes |
Metastasis |
Typical Treatment |
5-Year Survival Rate |
|
1A |
≤3 cm |
None |
None |
Surgery / SBRT |
~92% |
|
1B |
3-4 cm |
None |
None |
Surgery / Chemo |
~68% |
|
2A |
4-5 cm |
Limited |
None |
Surgery + Chemo |
~53-60% |
|
2B |
5-7 cm |
Limited |
None |
Surgery + Radiation |
~35-46% |
|
3A |
Any |
Same-side nodes |
None |
Chemo + Radiation |
~19-24% |
|
3B/3C |
Any |
Opposite-side nodes |
None |
Chemo + Radiation + Immunotherapy |
~10-13% |
|
4A |
Any |
Any |
1 distant site |
Systemic therapy |
~10% |
|
4B |
Any |
Any |
Multiple sites |
Systemic therapy |
~1-7% |
How Is Small Cell Lung Cancer (SCLC) Staged?
SCLC makes up about 15 percent of lung cancer cases. It grows and spreads faster than NSCLC, which is why its staging system is simpler and built around treatment decisions rather than precise anatomical measurements.
SCLC uses a two-stage system:
Limited Stage - Here, the cancer is confined to one side of the chest and can be treated within a single radiation field. The tumor may involve nearby lymph nodes on the same side. About one-third of SCLC patients are diagnosed at this stage.
Treatment: Concurrent chemotherapy and radiation therapy. Prophylactic cranial irradiation (PCI) may be added to reduce the risk of brain metastasis.
Extensive Stage: Here, the cancer has spread beyond one side of the chest, including to the opposite lung, fluid around the lungs, or distant organs. Most SCLC patients, approximately 60 to 70 percent, are diagnosed at the extensive stage.
Treatment: Chemotherapy combined with immunotherapy is now the standard, following approvals based on drugs' clinical trial data. Radiation for symptom control may also be used.
How to Find Out Your Lung Cancer Stage?
The Diagnostic Process
Staging is not a single test. There are a few lung cancer diagnostic tests that help figure out if the affected person has the disease or not.
It is a process involving multiple steps:
- Imaging: A chest and abdominal CT scan is the first step. A PET scan is used to identify areas of metabolic activity that may indicate cancer spread.
- Brain MRI: This is typically recommended when the cancer has reached stage 3 or stage 4, or when a patient is showing neurological symptoms. In earlier stages, doctors may still order it depending on the clinical picture and their own judgment.
- Biopsy: A small tissue sample is taken to confirm what type of cancer it is. For NSCLC specifically, this sample also allows doctors to run biomarker testing, which looks for specific mutations like EGFR, ALK, ROS1, and PD-L1 expression. These results play a big role in deciding which treatment will work best for that particular patient.
- Bronchoscopy or Mediastinoscopy: Used to sample lymph nodes in the chest to assess node involvement.
- Bone Scan or Additional Imaging: Ordered when symptoms suggest possible bone metastasis.
Once all results are collected, a multidisciplinary team, including an oncologist, thoracic surgeon, radiation oncologist, and radiologist, reviews the findings and assigns a final stage.
When to Seek a Second Opinion on Staging
Staging decisions, especially at stages 2B, 3A, and 3B, are not always straightforward. Borderline cases involve judgment calls about lymph node involvement and tumor resectability that different specialists may interpret differently.
The National Comprehensive Cancer Network (NCCN) recommends that all lung cancer patients have their case reviewed by a multidisciplinary tumor board before starting treatment. Major academic cancer centers with dedicated thoracic oncology programs routinely review complex staging cases from other institutions.
Getting a second opinion does not delay care in most situations, and it can significantly change the treatment plan for Stage 3 patients where the line between resectable and unresectable disease is thin.
Understand Your Stage, Then Ask the Right Questions
Knowing your lung cancer stage is the starting point, not the final word. The stage tells your care team where the cancer is and how far it has spread. From there, biomarker results, performance status, and overall health all influence what treatment makes sense.
If you or a family member has been recently diagnosed, ask your oncologist these four questions:
- What is the clinical stage, and how was it determined?
- Has biomarker testing been completed, and what were the results?
- Was my case reviewed by a multidisciplinary tumor board?
- Am I eligible for any clinical trials based on my stage and molecular profile?
Conclusion
A lung cancer diagnosis is difficult, but knowing your stage makes the path forward clearer. It is not a final verdict. It is a starting point that helps your care team plan the right treatment and helps you ask better questions. Treatment has come a long way. Targeted therapies, immunotherapy, and early detection through low-dose CT screening have improved outcomes across all stages. Staying informed and involved in your care genuinely makes a difference. No two cases are identical, and the right specialist team can help enlighten you with treatments you may not even know exist.
Do not navigate this alone. Explore our resources on lung cancer treatments, clinical trials, and specialist care options near you. Book a consultation with an oncologist and take your next step with confidence.
Key Takeaways:
- Lung cancer is categorized into two main types: Non-small cell lung cancer and small cell lung cancer, each with its own staging system.
- NSCLC uses a four-stage system (stages 1-4); SCLC uses a two-stage system: limited and extensive.
- Doctors use the TNM framework, tumor size, node involvement, and metastasis to assign a stage. Stage 1 is the most treatable; stage 4 means the cancer has spread to other vital organs.
- The 5-year survival rate for Stage 1 NSCLC can exceed 60%, whereas the survival rate for Stage 4 is around 7-8%.
- Early detection through low-dose CT screening significantly improves the chances of catching lung cancer at a lower stage.
