Table of Contents
- 1What Does a Stage 3 Endometrial Cancer Diagnosis Actually Mean?
- 2The Four Substages and Why They Matter More Than the Stage Number
- 3Symptoms That Bring Most Patients to Diagnosis
- 4Surgery: Why Less Invasive Options Are Not Sufficient at Stage 3
- 5Chemotherapy and Radiation: Why Both Are Needed
- 6Survival by Substage
- 7What to Watch for After Treatment?
- 8Conclusion
- 9Key Takeaways
What Does a Stage 3 Endometrial Cancer Diagnosis Actually Mean?
Each family’s response to the diagnosis of endometrial cancer stage 3 will vary. There will be families who will receive their diagnosis with the results of the surgery they have had three times over. Other families will receive theirs with just one sentence: the doctor said, “It has spread.” One of the most frequent questions that will emerge at this point is not regarding the chances of survival, but rather, "Is there no other way around it?"
Stage 3 endometrial cancer means the cancer has grown beyond the uterus but has not reached the bladder, rectum, or distant organs like the lungs or liver. It is locally advanced and serious. But in most cases, it is treatable. The five-year relative survival rate for regional endometrial cancer is approximately 70%, according to the American Cancer Society, and that number improves meaningfully when surgery is combined with both chemotherapy and radiation.
The Four Substages and Why They Matter More Than the Stage Number
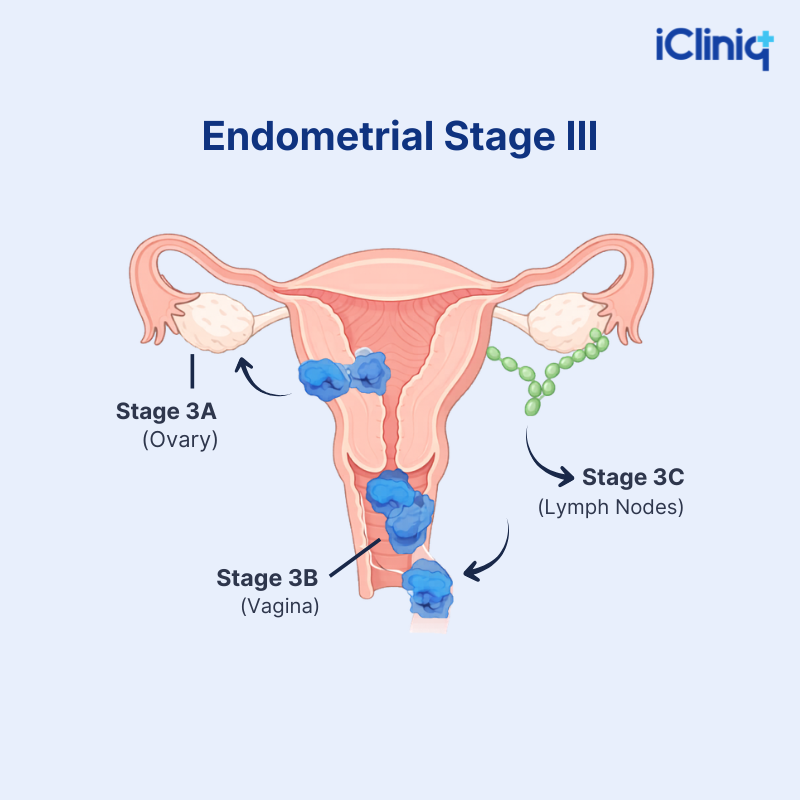
Stage 3 is not one situation. There are four substages, each describing exactly where the cancer has spread. Treatment, radiation field, and prognosis all change accordingly with the substage, which is why the substage is the first thing an oncologist looks for in the pathology report, not the stage number alone.
|
Substage |
What Is Involved |
|
IIIA |
Cancer has grown through the outer uterine wall or reached the ovaries and fallopian tubes. |
|
IIIB |
Cancer has spread to the vagina or parametrium (connective tissue surrounding the uterus). This is the least common, and 4% of stage 3 cases. |
|
IIIC1 |
Cancer cells have reached the pelvic lymph nodes but not the para-aortic lymph nodes. |
|
IIIC2 |
Cancer has spread to the para-aortic lymph nodes, with or without pelvic node involvement, and the prognosis is most cautious. |
Staging is confirmed at surgery through pathology of the removed tissue, not imaging alone. This is why the substage sometimes changes after surgery. The staging may assign IIIA after removal of a few lymph nodes; however, later on, with fuller nodal assessment, it may be revised to IIIC1. That is not an error; it is more complete information, and it changes what treatment is needed.
Symptoms That Bring Most Patients to Diagnosis
Bleeding from the vagina, especially in cases where there has been twelve months without a menstrual cycle, forms the basis for detecting most endometrial cancers. However, it often emerges that the patient had months of abnormal bleeding due to perimenopause before imaging.
By stage 3, additional symptoms often appear:
-
Pelvic pain or pressure that does not resolve.
-
Abnormal discharge from the vaginas, which can be watery, pink, or blood-stained.
-
Unexpected loss of weight.
-
One-sided leg swelling, which can indicate pelvic lymph node obstruction.
A delay between the first symptom and diagnosis is a consistent pattern in consultations, bleeding dismissed as hormonal, and pain attributed to musculoskeletal causes. Post-menopausal bleeding should never be investigated later. It should be investigated now.
Surgery: Why Less Invasive Options Are Not Sufficient at Stage 3
Many patients tend to inquire about the possibility of an alternative approach that is less invasive during pre-operative consultations. The straightforward reply would be that it is not feasible since, in stage 3, the cancer will have advanced past the uterine wall.
The standard surgical approach involves:
-
Radical Hysterectomy: In this, your doctor may remove the uterus, cervix, upper vagina, and parametrium.
-
Bilateral Salpingo-oophorectomy: In this procedure, your doctor removes both fallopian tubes and ovaries.
-
Lymph Node Dissection: To assess and remove affected nodes
Surgery is the first step in a multimodal plan, not the complete plan. One conversation that must happen before surgery, particularly for younger patients: this procedure ends fertility permanently. For a woman in her late thirties, this is not a side note; it is a central part of informed consent that must be discussed with the treating doctor before proceeding, not after.
Our patients recently asked: Why is a hysterectomy needed in stage 3 endometrial cancer?
At stage 3, the cancer has already spread beyond the uterine wall, making less invasive options insufficient to control it. A radical hysterectomy combined with lymph node removal gives the best chance of clearing all visible disease before chemotherapy and radiation begin. Read the full consultation →
Chemotherapy and Radiation: Why Both Are Needed
A question that comes up consistently after surgery: "We thought the uterus being removed meant the cancer was gone. Why is radiation also needed?"
Surgery removes everything visible. It cannot reach microscopic cancer cells that have already traveled beyond the surgical margins, cells not detectable on any scan, not visible in any pathology report. Radiation destroys these cells. It is an adjuvant treatment, preventive, not a sign that surgery was incomplete.
Chemotherapy: Medicines like Carboplatin and Paclitaxel, given intravenously across six cycles after surgery.
Common side effects include:
-
Nausea and fatigue are most pronounced in the five to ten days after each infusion.
-
The sensation of peripheral neuropathy may present itself in the form of numbness or tingling sensations in hands and feet.
-
Temporary loss of hair.
-
Increased risk of infections due to low white blood cell counts.
Radiation: This is done for five to six days, and the course takes four to six months. The patient may receive vaginal brachytherapy as an additional treatment for reducing recurrence in the vaginal cuff area.
The side effects of this process involve the following:
-
Inflammation of the bowel.
-
Burning sensation on urination.
-
Fatigue.
-
The vaginal region may become dry and constricted, which may be treated with dilators and lubricants.
The rationale behind combining these treatments is very clear. Patients who underwent both chemotherapy and radiation therapy had a five-year survival rate of 65.2%, as opposed to patients who took just one of the two treatments (NCBI, 2023).
The most common misunderstanding we see after surgery: the uterus being removed means the cancer is gone. A 60-year-old patient's family came to us with exactly this assumption, and it is an understandable one. Surgery removes everything visible. What it cannot do is reach microscopic cancer cells that have already traveled beyond the surgical margins, cells that leave no trace on any scan or pathology report. Radiation exists specifically for this. It is not a second treatment for the remaining visible disease. It is the treatment for what surgery, by its nature, cannot see.
Radiation is not automatic for every endometrial cancer patient. Whether it is needed for lower-risk cases depends on specific findings in the surgical pathology report, depth of muscle invasion, lymphovascular space invasion, lymph node status, not the biopsy grade alone. The pathology report drives this decision.
Whether radiation applies to your mother's specific case depends on what the surgical pathology report says, not the biopsy grade assigned before surgery. One family worked through this exact decision here. The findings that matter are the depth of muscle invasion, lymphovascular space invasion, and lymph node status. A grade 2 tumor confined to the uterus with minimal invasion and clean lymph nodes may not need radiation at all. The pathology report after surgery is the document that answers this question, not the grade on the biopsy report.
Survival by Substage
|
Substage |
5-Year Overall Survival (with adjuvant therapy) |
|
IIIA |
58 to 67% |
|
IIIB |
58% |
|
IIIC1 |
49 to 57% |
|
IIIC2 |
41 to 48% |
Sources: NCBI 2023, published surgical registry data.
The statistics apply to groups, not individuals. The survival rate after five years at even stage IIIC2 can be over 40% when a combined approach is used. Stage 3 cancer should not be an excuse for discontinuing treatment.
One point worth stating plainly for patients who have read alarming statistics online about carcinosarcoma: Stage 3C is not considered an extremely dangerous stage because treatment outcomes can be very good. The reassuring part is that there is no spread outside the uterus or the pelvic area. When the cancer is still confined to the pelvis, it can be controlled quite effectively.
Carcinosarcoma is a more aggressive subtype than standard endometrioid cancer. It carries a lower stage-for-stage survival rate, but even with this diagnosis and at an older age, treatment can still be highly effective. Patients with this subtype deserve to know this directly rather than be given statistics that apply to a different histological category.
Our patients recently asked, "Can stage 3C endometrial carcinosarcoma be fatal at age 59?"
Stage 3C is not considered an extremely dangerous stage - the cancer is still confined to the pelvis, where it can be controlled effectively with surgery, radiation, and chemotherapy. Even at an older age, treatment can still be highly effective with good outcomes. Read the full consultation →
What to Watch for After Treatment?
Roughly 35 to 50% of patients with stage 3 disease experience recurrence, most often within the first two to three years. The most common sites are the vaginal cuff, pelvic lymph nodes, and, less frequently, distant organs.
Monitoring Schedule:
-
Pelvic examination every three to six months within the first two years, followed by yearly exams thereafter.
-
Results of CA-125 tests at each appointment.
-
Imaging studies such as computed tomography/positron emission tomography (CT/PET scans) are performed only when there are symptoms or elevated CA-125 levels.
Signs that should not wait for the next scheduled appointment:
-
Any vaginal bleeding after a hysterectomy.
-
New one-sided leg swelling after treatment ends.
-
Persistent back or flank pain that does not respond to standard pain relief.
-
CA-125 that doubles between two consecutive tests, even within the normal range.
-
New urinary symptoms like blood in the urine or difficulty passing urine after pelvic radiation has finished.
Most vaginal cuff recurrences are detected on pelvic examination before imaging would have found them. Attending every appointment matters more than requesting routine scans between visits.
Conclusion
Stage 3 endometrial carcinoma involves four sub-stages, multiple histological types, and a treatment program that must fit perfectly with the stage of the disease. The patients who perform the best are those who know their exact sub-stage, know the reasons for each part of the treatment program, complete the whole program when eligible, and attend all follow-up visits.
Families who ask questions before agreeing to treatment, "Why this surgery? Is radiation really necessary?" What does stage 3 mean for her specifically? ", are asking exactly the right questions. Informed consent is not delayed. It is the foundation of every good treatment decision.
For a second opinion on a stage 3 endometrial cancer diagnosis, pathology report, or treatment plan, consult a cancer specialist.
Key Takeaways
-
Stage 3 endometrial cancer is locally advanced, which has spread beyond the uterus into the pelvis or regional lymph nodes but has not reached distant organs.
-
Four substages exist, IIIA through IIIC2, each changing the treatment plan, radiation field, and prognosis.
-
Surgery followed by both chemotherapy and radiation gives better survival than either alone. The five-year overall survival rate is 70% with combination therapy (NCBI, 2023).
-
Radiation after surgery is preventive. It targets microscopic cancer cells that surgery cannot reach and the remaining invisible disease.
-
Surveillance every three to six months for two years is standard; most recurrences are found on pelvic examination, not routine scanning.

